As the popularity of explant procedures increases, we are seeing a corresponding increase in the number of ladies who have unsatisfactory outcomes from their explant procedures. Patients are presenting seeking correction as they neither look, nor feel right. They understand that something is wrong, but they aren’t sure what.
COSTS:
Plastic Surgeon’s fee: requires individualised quotations. From $12,500.
Associated item numbers: 45551 may apply (if total capsulectomy not performed with original explant).
Unfortunately, for patients who have had explant surgery with item number 45551 previously applied (and where the surgeon actually performed a complete capsulectomy), further item numbers may not be applicable for surgery to correct poor cosmetic outcomes. This does require careful assessment on a case-by-case basis.
LENGTH OF PROCEDURE/ HOSPITAL STAY:
2.5-4.5hrs
Day surgery for most patients.
Dr Campbell-Lloyd does NOT use drains after capsulectomy or for revision explant procedures.
Important Information:
Typically, dissatisfaction with explant outcomes relates to the shape of the breast, although patients often can't quite describe what it is they don't like. Frequently, these ladies will be requesting fat transfer to "fix" their concerns (often because that has been presented to them as some sort of solution by their previous surgeon). Unfortunately, there is a lot more required in these cases, and it is important to understand the underlying cause of poor outcomes after explant.
Dr Campbell-Lloyd has previously written about "explant related harm" and that touches on some similar topics. You can also find a long-form exploration of Explant Revision Surgery over on our blog where we discuss what comprises a "good" explant (versus a bad one), the causes of poor outcomes after explant surgery, and the ways we we correct those poor outcomes.
We do encourage all patients considering explant revision to discuss their concerns with the original explanting surgeon. Some patients don't feel comfortable going back to see their original surgeon. However, most patients come to us seeking our advice on explant revision because they have followed-up with their original surgeon and haven't been happy with the answers provided when questioning their outcome.
Poor outcomes after explant are associated with a few common issues. Often a "bad" explant presents with residual implant capsules and the deforming force of an un-repaired Pectoralis major muscle. Addressing these points plays a primary role in Explant Revision surgery.
When we perform explant revision procedures, we are generally trying to do the things that should have been done at the time of the original explant procedure. So when considering how we revise poor outcomes after explant, we will mostly find ourselves addressing the steps in an explant procedure that should have been done in the first place.
"Completion" capsulectomy
In many cases of explant revision, there will be residual implant capsule (that wasn't removed at the previous explant procedure). In other cases, the surgeon did perform a total capsulectomy, but we find that a so-called pseudocapsule has formed after the explant, which could theoretically arise due to either a post-operative chronic seroma/fluid collection (which the body then forms a capsule around), or due to ongoing movement of the unrepaired Pec muscle (which stimulates the formation of the pseudocapsule).

Regardless, any form of capsule that remains must be removed to facilitate the muscle repair that then takes a primary role in most explant revision cases.
The popular idea that the muscle and the breast will just "stick back down" onto the chest wall is incorrect; at least, it is incorrect to assume that things will stick back down where they should. We find that when tissues have re-adhered to the chest wall, the muscle normally remains sitting too high on the chest, and the breast tissue that sticks down is in the lower, inner portion of the breast. This is precisely what leads to the common "concave" appearance of the lower part of the breast after explant. These ladies will also have persisting animation deformity arising from the high-riding pec major muscle.
Correcting the breast crease and scar placement
Many ladies will present after explant with two related issues: the breast fold/crease will look unnaturally high, and the scars are visible a long way below the breast fold. A primary goal of explant revision surgery is to correct the breast crease (which involves repositioning the breast tissue downwards, back into the lower pole of the breast where it belongs), and securing the scar upwards into the breast crease (using so-called "internal bra" suture techniques).
These two aspects of Explant revision surgery really do go hand-in-hand, and each relies on the other for an acceptable outcome.
Repairing the Pectoralis major muscle
Muscle repair is the single most important step we take in Explant Revision procedures (for women who had dual-plane or under-the-muscle breast implants), because an unrepaired Pec muscle plays a central role in deforming the breast after explant surgery.
Muscle repair is the single most important step in Explant Revision procedures.
Whilst an animation deformity can be elicited with muscle contraction during activity, even at rest (and without contracting the Pec muscle) the unrepaired muscle is responsible for the lower pole concave deformity, the superior malposition of the breast fold, and widening of the cleavage that we so often see after poorly done explant procedures. Repairing the muscle addresses all of these issues.
Reconstructing the breast "boundaries"
Breast augmentation procedures often involve deliberate destruction or violation of the anatomical breast boundaries, which Dr Campbell-Lloyd has discussed in a previous article.
The 3 breast boundaries that must be addressed are the cleavage, the inframammary crease/breast fold, and the (less defined) outer breast boundary. By controlling the breast boundaries, we gain the ability to more accurately determine exactly where the breast tissue sits, and in small-breasted women, this also contributes to overcoming the "thinning" of the breast tissue that can arise with large implants.
Fundamentally, the breast boundaries must be rebuilt in order to stabilise the position of the breast tissue, which is necessary to prevent or address the typical contour deformities we encounter after poorly performed explant procedures.
Correcting the breast contour (especially in the lower pole)
The breast contour after explant can be distorted or deformed by a range of factors, and addressing each of these is essential in Explant Revision surgery.
The classic contour deformities include lower pole "concavity" (which is a consequence of an unrepaired Pec muscle) and nipple "retraction" or a horizontal crease across the middle of the breast (which is most commonly seen after the removal of large prepectoral implants).
Adding volume to the breast
In many cases, adding some volume back into the breast with fat transfer can help to improve the aesthetic result of Explant Revision surgery. However, fat transfer alone is NEVER the solution to problems like lower pole concavity or central depressions. Fat transfer is a wonderful technique but it can only work correctly if all of the steps mentioned above have been addressed first.
Mastopexy
A related but slightly separate issue is when we see poor outcomes after explant because the patient needed a mastopexy at the time of her explant but was told that her breast would "tighten up" without further intervention.
We consider this a separate issue because this has more to do with surgical judgement and planning, rather than having to do with the execution of the explant itself.
There are two possible scenarios here: 1) a lady with a larger breast which has fallen over the front of her implants; or 2) a lady with a smaller breast who had very large implants which have stretched the skin of the breast. Admittedly, determining exactly who needs a mastopexy and who doesn't can be challenging.
The decision to do, or not to do a mastopexy is a key demonstration of a surgeon's experience with regards to explant procedures, and Dr Campbell-Lloyd has written about this previously in the context of ladies with small natural breasts that have been stretched by large implants.
It is possible to correct most of the problems seen after poorly performed explant surgery. It certainly isn't easy, and it seems a pity that a patient would have to go through two operations, when it could all have simply been done in one.
Residual capsules
Most patients will have been told they had their capsules "removed" by their original surgeon, but this seems often to not have been the case. The item number typically used for explant surgery (45551) stipulates that "at least half" of the capsule must be removed, but in our experience it appears that just the lower part of the anterior capsule (the part between the bottom of the Pec muscle and the breast crease) has been removed (which is perhaps 25% of the total capsule) and the remainder left behind.
There is a persistent myth that thin capsules will just magically "reabsorb", and many surgeons still think that the capsule somehow provides blood supply to the breast tissue, and that removal of the capsule could therefore cause tissue death or limit the ability to manipulate the breast (as in a mastopexy) or perform fat transfer. Whilst neither of these things is true, the beliefs remain pervasive.
Residual capsules are a problem for patients. Obviously, many ladies having explant surgery are concerned about whether their capsules could be contributing to functional symptoms (like Breast implant illness - however, it must be stressed that there is absolutely no evidence currently to support that idea; the evidence would currently suggest that removal of implants alone, irrespective of how much capsule is removed, is likely to result in improvement of BII symptoms). Other ladies have pain associated with their implant capsules, especially if they are contracted (which may also be associated with the scar capsule irritating surrounding nerves, either physically or due to inflammation). And from our perspective, the capsule totally prevents proper repair and reattachment of the Pectoralis major muscle, which is vital step in achieving good outcomes after explant surgery.
Dr Campbell-Lloyd considers the removal of any residual capsule is a necessary step in Explant Revision Surgery.
Scar malposition
A low scar that sits below the breast crease, rather than being carefully placed and hidden in a well-defined breast crease is one of the most common features of poor outcomes after explant surgery, and it is related to a couple of other problems. The scar malposition arises due to a failure to stabilise the inframmamary fold, a failure to correctly reposition the breast tissue into the lower pole, and a failure to manage the underlying Pec major muscle. All three of these issues must be addressed if we want the scar to end up well positioned and neatly hidden in the breast crease.
Widened cleavage
The position of the breast tissue in the cleavage is determined by the the fact that it is attached to the underlying Pec major muscle. Because the muscle is frequently released from the sternum at the time of the original breast augmentation - this is something we discuss as being one of the many flaws of the "dual-plane" technique - or potentially at the time of the previous explant, then the management of a widened cleavage normally involves a combination of repairing the muscle onto the sternum, internally suturing the breast tissues to address any thinning of the tissue, and fat transfer.
Animation deformity
Just as the muscle is responsible for animation deformity for ladies who have breast implants, once the implant is removed the muscle can still cause dynamic deformation of the overlying breast tissue if it hasn't been properly repaired.
The muscle must be pulled not just downwards (and reattached to the ribs), but also inwards towards the cleavage (and reattached to the sternum) in order to minimise the risk of animation after explant.
One of the unique problems with the dual-plane breast augmentation technique (as it relates to explant surgery) is that the muscle is released from the overlying breast tissue. This creates a major challenge as it relates to animation deformity after explant, even when the muscle is repaired.
In the normal breast, there is a "gliding" layer between the breast and the muscle. This gliding layer allows the muscle to move independently of the breast tissue, so that the breast doesn't move when the muscle contracts. Once a surgeon has entered that layer to release the muscle off the breast in a dual-plane augmentation, this gliding layer is destroyed and is replaced by thick, sticky scar. And once it's gone, there is no getting that gliding layer back.
So even when we do repair the muscle (and this is mostly an issue for the small breasted ladies), because the gliding layer is lost, when the breast tissue heals back onto the muscle there will still be some tendency for the lower part of the breast to move when the muscle contracts, even though the muscle is properly anchored onto the ribs. This can be a challenging problem with explant, and it can be an even more challenging problem when we do explant revisions.
Lower pole concavity
Lower pole concavity is the most immediately obvious sign of a poorly performed explant procedure. This fundamentally relates to an unrepaired Pec muscle, and thus it is something we really only see for ladies whose implants were under the muscle. If the muscle is not repaired, and is allowed to pull up towards the shoulder, it drags the overlying breast tissue with it creating the classic "empty" lower pole which is a significant aesthetic issue.
We see a lot of ladies who have been told that fat transfer is the solution to this problem. Unfortunately, on its own, fat transfer is not the solution. It may be a useful addition, but without a proper muscle repair, the lower pole concavity will persist.
Central concavity or nipple inversion
More commonly an issue for ladies who had prepectoral implants, central contour deformities of the breast - which present as a horizontal crease across the breast, or a tethered scar associated with a nipple and areola that appears to be "sucked inwards" - can be very challenging to address secondarily. This may require a number of different techniques, including releasing tethering scars, using "internal mastopexy" techniques, fat transfer, or performing a formal mastopexy (with autoaugmentation) to overcome the problem. This is one of the most challenging issues to deal with for small breasted ladies.
Sagging or deflated breasts after explant surgery
The question of whether a woman requires a mastopexy at the time of explant can be challenging. Whilst there can be some limited expectation that the breast tissues will "tighten" after removal of implants, this is an unpredictable process, and any surgeon performing explant procedures needs to be capable of accurately judging which patients do or don't require a mastopexy to avoid breast deformity after explant.
When performing explant revision, mastopexy can be performed at the same time as the other necessary steps to correct any breast distortion or deformity.
The outcome of explant revision surgery should ideally be a natural breast shape with correction of the presenting concerns, whether that is a scar below/out of the breast crease, contour issues on the breast, or animation deformities.
However, it is important to understand that “fixing” a poorly performed explant is much harder than doing it correctly the first time, and therefore there will be some patients in whom we cannot completely correct every issue. Some patients may require additional procedures – such as further fat transfer – to achieve the goal of restoring their breast shape and contour.
The appearance of the breast and the nature of the recovery can vary according to exactly what has been done, however there are a couple of common features that will apply to nearly all explant revision patients.
Firstly, you should expect that the incisions required for the revision surgery will be a bit longer than the original explant. It is typically the case that when an explant has been done poorly, the surgeon was operating through a limited incision (because they had no intention of managing the lower pole of the breast, doing a complete capsulectomy, or performing a muscle repair for example, all of which demand a longer incision to be done well).
Secondly, you should expect that the revision surgery will be associated with more discomfort than the original surgery. This is often associated with the capsulectomy and muscle repair (versus when those steps are not performed) but also because many of our explant revision patients will have additional procedures like fat transfer.
Thirdly, you should expect a stricter period of reduced activity in your recovery. Because of the complexity of this surgery, and the fact that we don’t use drains, we do demand compliance with strict activity limitations to ensure a safe recovery (and hence, a good aesthetic outcome!).
Post-operative details:
All sutures are dissolving sutures, under the skin. A layer of glue is then applied to any incisions. There are no “sticky” dressings applied which can cause irritation and prevent showering.
After explant revision surgery, patients are discharged home with a surgical compression bra which must be worn at all times for the first 6 weeks. If fat transfer has been performed, a lower body compression garment is also required.
Patients are discharged with antibiotic tablets, and pain-relief medications.
Patients are discharged home with detailed instructions. The instructions include emergency contact details for Dr Campbell-Lloyd.
Routine follow-up appointments are typically made for (this can vary for interstate/international patients):
Patients are then seen every 4-6 months as scars fade. Most patients are stable and are discharged at 12-18 months post-op, however we are happy to see any of our patients in an ongoing fashion.
We do not charge for post-op consultations.
The nature of this surgery is such that patients should expect to require pain relief medication for at least the first 2-3 weeks. Some patients will require simple pain relief (such as Nurofen) on occasion for up to 6 weeks as they increase activity. The need for pain relief will be dependent on the original surgery performed, the amount of "damage" to the normal anatomy that we have to correct, the presence of residual capsules, and a patient's level of activity after surgery.
It is vital to maintain a decreased level of activity for 6 weeks after surgery to reduce pain and swelling, prevent fluid collections, and to ensure that the muscle repair is not inflamed or aggravated.
It will take at least 3-4 months for full recovery. Final results can only be appreciated after that time, once scars have softened and relaxed. Scars may only fade after 6-12 months on the breast.
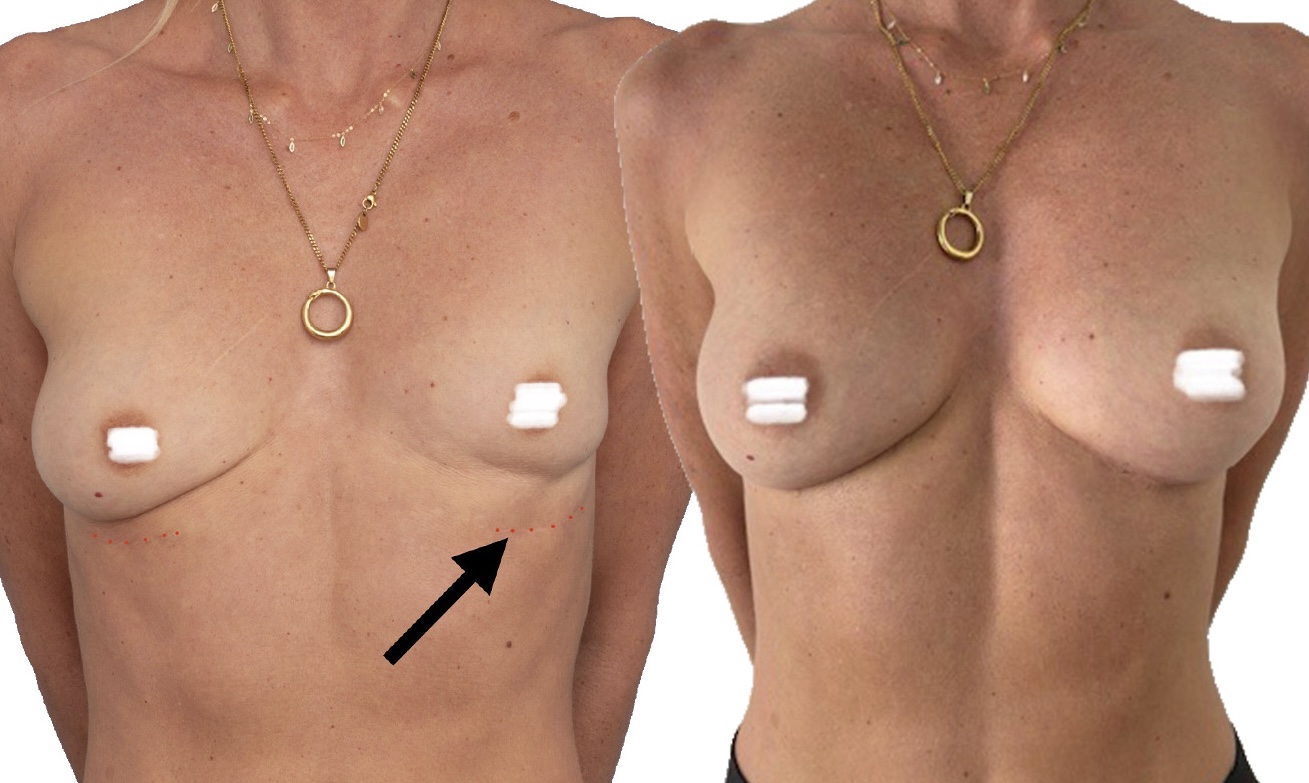


Some examples of explant revision/correction procedures done by Dr Campbell-Lloyd. You can follow us on instagram @drcampbelllloyd to see more.